Quakefire
-
Posts
261 -
Joined
-
Last visited
-
Days Won
3
3 Followers



Recent Profile Visitors
12,407 profile views



Quakefire's Achievements
")




-
I’m sad to share the passing of Marc Moebis, better known as Mobey on this site. Alberta has lost a great paramedic and mentor
-
Nerve Blocks and Sutures? That would probably decrease our number of transports a fair bit. 5 minutes is a very long time, but sometimes IO is the only way to go, never want to have an exj as my only option on a 400 pound patient. Unfortunately benzos are not a common option for pain control for us. Our protocol requires at least 2 doses of a narcotic pain killer with no relief (and usually right up to our max dose 250mcg of Fentanyl or 10mg Morphine) before we can request versed or ketamine for pain from our medical control.
-
One of my partners is getting ready to go back to school to become an Advanced Care Paramedic, and she has been doing an online A&P course ahead of time for a little extra study time during the course and she asked an interesting question. According to her text books the only place that has any nerve endings is in the periosteum, and yet we teach that the pain of insertion of an IO is much lower than the pain from the infusion. So she asked where the infusion pain comes from and I haven't the foggiest idea. I know there are people here much smarter than me so can anyone answer this question? Dan
-
I still lurk from time to time. Not quite 10 years but I do remember the "glory days"
-
This is only the second patient I have encountered with an acute inferior MI, last one was declining very rapidly so I was being cautious with anything that might cause hemodynamic compromise, this in addition to the fact that when asked the patient stated she has never had morphine before. As a side note, I never placed defib pads on this patient. I explained to her what was happening and what might have to happen, but she was quite anxious and I had very quick access to our monitor so I felt that any decrease in her anxiety was also a good thing. I doubt that I would have had to pace her at any point, as she is far more likely to progress into a vfib.
-
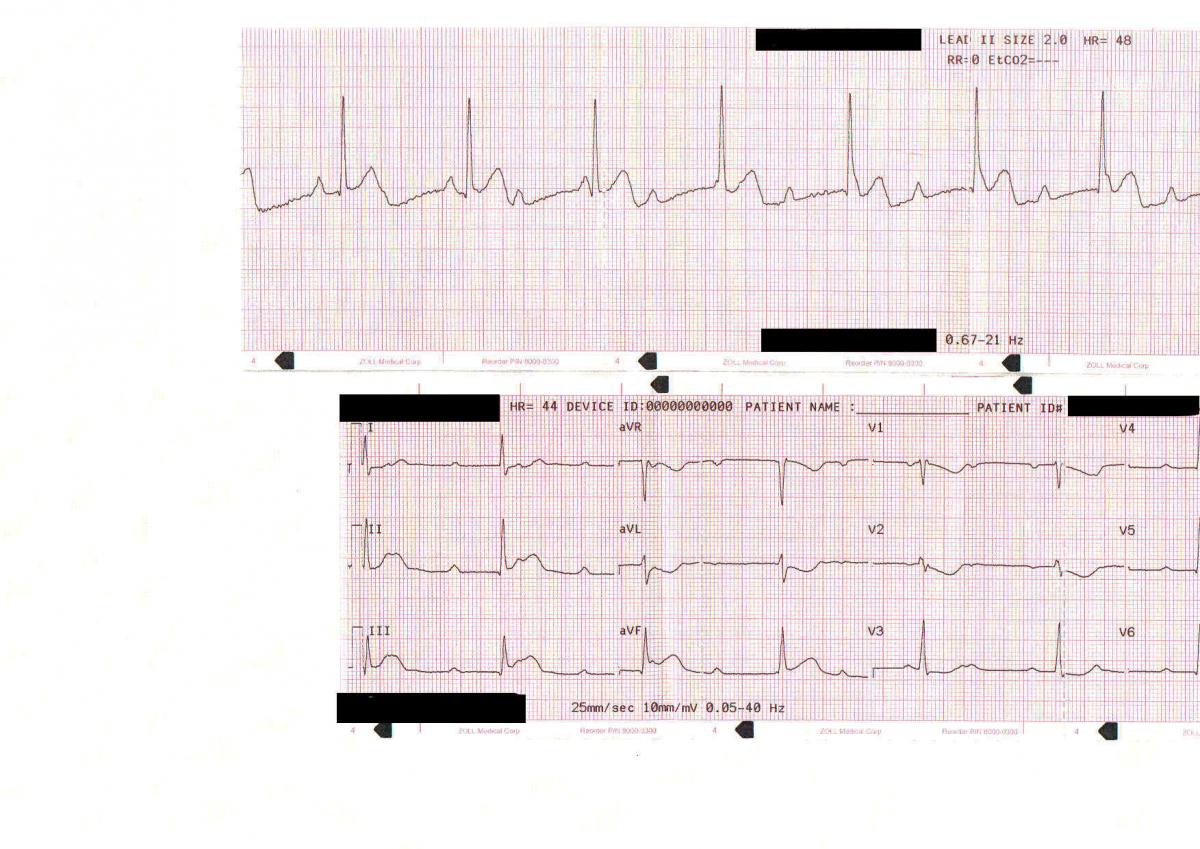
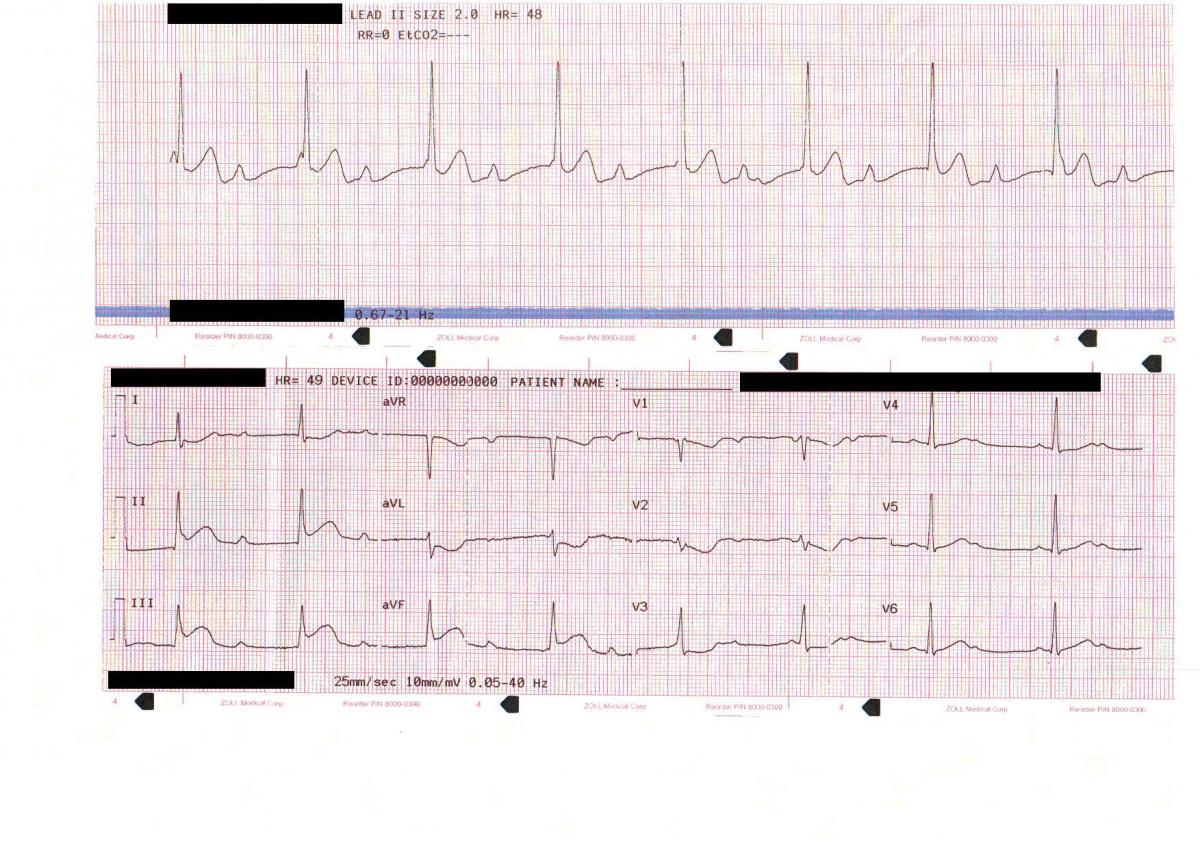
Our treatment was pretty simple. I cheated a little bit with the ECG's, the first 3-lead and the first 12 lead are 10 minutes apart, the second 3 lead was 7 minutes after that and the final 12 lead was 30 minutes after the initial 12 lead. ASA, O2 with nasal cannula at 4lpm, 18g IV with NS TKO. I gave two 2mg doses of Morphine about 15 minutes apart being mindful of her BP which didn't change for us. This only dropped her pain to a 5/10 I really don't see this patient as a symptomatic bradycardia as the lethargy was consistent with her normal use of the sleep aid (Zopiclone). The main issue I have with using dopamine is the inotropic and chronotropic effects on the heart. I dont want to make a damaged heart work harder (plus dopamine isnt in our protocol for that) Nitro is contraindicated in this patient as per our protocols. Pt maintained her GCS, BP and vitals throughout the transport to the recieving hospital and into the cath lab 10 minutes later. Pt had a 100% occlusion of the RCA, once cleared and stented the 3rd degree AV block resolved and the patient left the CCU into a cardiac ward within 3 days. Thanks for playing!
-
Follow up 12 lead and 3 lead after ASA, Morphine, O2 Edit for Vitals: No change in vitals, pulse remains 45, BP 124/68 RR 18, SpO2 98% Pain 5/10 after 4mg Morphine IVP

-
I did see that, just looking for a diagnosis from that. Any further treatment?
-
Ok, to consolidate everyones treatment We are now enroute to the Cardiac Center, about 40 minutes transport, we have O2, a NS line, 3-lead and 12 lead, and quick combos in place. STEMI alert has been called. Haven't seen a interpretation of the 3-lead, and no one has has actually said what kind of MI the 12 lead shows And just you in the back, in the event that she goes into arrest, you have access to a Zoll Autopulse.
-
The fall as described to dispatch was when the patient dropped herself onto the bed, no syncope. No prehospital fibrolytics yet supposed to be in the pipeline. Also no pressors except for severe sepsis Home hospital is 20 minutes away, Lab, X-Ray, ECG "Big City Hospital" is 40 minutes away, Cardiac specialty, Cath lab, Cardiac Sx and CCU. This hospital has a STEMI alert protocol Of course two hospitals are in opposite directions so transfer time is 60min. Rotary wing is not available at this time
-
Oh and here is the requested 3-lead and 12-lead

-
I went to SIAST as a Sask trained and registered PCP for my Advanced care Paramedic. I had two PCP's from BC in my class who had issues with the JI because of the strike. Both passed one is employed with BCAS the other stayed in Saskatchewan. As the courses and their content is always changing I can't comment specifically to the course now except that it is still a CMA accredited program. As HellsBells stated SIAST is a full time program M-F 9-4:30 in either Regina or Saskatoon with class sizes of about 30, Practicum placements throughout the province. minimum requirements are listed in the course info. Passing requires passing the course as well as your practicum which is up to your preceptors and practicum coordinator. As for a lack of a strict selection process, students tend to get weeded out by exams and through practicum, no one is guaranteed a pass
-
No allergies known, Zopiclone is a PRN medication but no excessive amount of medication is missing from the bottle (not empty and refilled two days ago kinda thing) Dose taken is normal and listed on bottle. Fall described as "plop" on the bed BGL 6.8 mmol/L (122.4 mg/dL)
-
It sounds like only the newer style AEDs and possibly the R-Series are capable of determining what pads are attached to the monitor
-
Daughter stated that the somnolence and CNS presentation is normal for patient when on this medication. I will post a 3 and a 12 lead in the morning probably because I don't have them with me at the moment Sent from my iPhone using Tapatalk