


Ace844
-
Posts
1,350 -
Joined
-
Last visited
Content Type
Profiles
Articles
Forums
Gallery
Downloads
Store
Posts posted by Ace844
-
-
Here's a link to their website: http://www.infrascanner.com/
-
"Grassroots..." Who woulda thunk..?
Here are the links::
Formation of a new EMS political action group
Detroit Screws Up Again, Kills Another Person
-
Grassroots level involvement? Good plan Ace. Now the lazy, scared, or indifferent among us have to make their voices heard. Letters to Congressmen and Senators people.
For admin:
If we put together a letter to Congress, could you post the links to the senators/representatives so we could do a mass mailing?
One voice type solidarity.
Interestingly enough I believe there is already one of those in existance as our distinguished colleagues "PRPG, et. al, and RidRyder911, et.al,DUSTDEVIL et.al.," {There are links ot these efforts post in "GAmedics recent thread; give me some time and I will post them here as well.} tried to do something quite similar, I would definatelty be interested in doing something of this nature, but the real question is will our peers who post here step up to the plate and participate; or will this be a poor showing which is embarrasing like before? LETS HEAR IT PEOPLE, ARE YOU IN??? "GAmedic,&others" heres your chance to back up what you say....
ACE
The most exciting phrase to hear in science, the one that heralds new discoveries, is not 'Eureka!' (I found it!) but 'That's funny ...'-- Isaac Asimov --
-
Hello Everyone,
I just found this interesting document and was wondering what you all thought of the points made here. Here's the link:
http://www.nemsma.org/Portals/3/NEMSMA%20P...l%20Support.pdf
OUT HERE,
ACE844
-
-
well at least it wasn't hemmhorraghic complications or a bunch of 70 yo's with spontaeous DIC...the incidence was pretty low, and I would be curious to find out what their pre-TPA EF, PMH, LDL, HDL, etc.. was, etc...it will be interesting to see what their new guidelines will be though.
-
I got me 1 o dem cryosuperprecipitators startek 5000 polypharmacy modulators, a roll cage, brushbars, 2 roatating light bars 10 LED strobes, 6 flashers, a pack of gum, 4 M tanks, a trauma or, all the koolaid i can drink, and 250-6gpm pumpms and tanks to cover all the bases....no bambulance is got dem dings.. oh and i forget me YAHOO MODEL 300 TYPE2 SIREEN...
SOUNDS LIK YAHOOOOOOO.......YYYYYYAAAAHHHHHOOOOOOO.....WHACKER....WHACKER...WOOP...WHOOP...
YAHOOO..............
-
So these were embolic cva's and thrombi thrown as a result of loosened atherosclerotic plaque...am I reading that correctly?
-
Nothing to increase the pucker factor like having your medical director running calls with you.

2nd year residents and nurse externs are doing ride time as we speak. By the time they are done, and actually making decisions or taking reports from us, they will have long forgotten what it was like. In the meantime, it is very useful.
The ER staff used to be required to do 12 hrs/year. Not a lot, but at least some. This has since gone away. RN's sucking up hospital department budgets on overtime, doing things that don't directly benefit the hospital isn't supported by administration much.
Course, everytime they ask why I've done something, I will offer to take them on some calls to show them what my work environment is like.

Actually it was great having the med director running calls because it had a 3 fold effect. 1.0 He got to know what it was like and expereince it on a regular basis 2.) got to know the crews and their abilities and disabilities 3.) Got to understand why we gave the ER staff crap soemtimes. There's nothing like having your med director tell a charge nurse to stop being a hag and pull her outta her A$$... yes that was an actual quote...and she deserved it to.. This particular doc used to be a medic before med school, so that helped as well..but I digress.
The nursing staff used to do it on a rotating basis about a shift or 2 a month soemtimes more, and it was on their time. We used to do the same in the ER and later the med director worked out a deal with the service whereby x many employees spent time in the ER as oppossed to doing a shift on a rotating basis. The medics did it in addition to mandatory rounds, etc.. It's soemthing I wish would happen more often.
Out here,
ACE844
-
Actually it was ME who resus'd the thread. I was going through ol BLS stuff and came across this which had been a topic in class recently.
Serves me right for using the search function?
Damned if you do...damned if you don't. Ace..I think you're just impossible to please.

I said it was you, and I was being facetious..JOKING....


 Mastabattas, HEREBY offically wins today sucessful use of the SEARCH button award!!
Mastabattas, HEREBY offically wins today sucessful use of the SEARCH button award!! 


-
How has that helped in your interactions at med-report, and transfer of pt.care?
"FL_Medic,"
"AZCEP" recently asked a question of this nature in one of the threads I think it was RSI but I am unsure, though he may know. To answer your question I have worked in systems where this was done but there are a few things to bear in mind and to consider. This can be a great tool, but there has to be a clear understanding on both sides of expectations, accptable dress, and what the 'riders' role if any beyond observation will be. This should be crystal clear and the circumastances and politicis as well as working relationships within the system and between the parties will differ so that is as detailed as I will get with that.
I personally have had docs and nurses ride both als and bls and as mentioned above their interaction ranged from stand in a corner in watch to 'running' the call just like we would do alone. Our medical director used to come out and ride at least 2- 12 hr shifts soemtimes more a month. These interactions helped our working relationships, as well as interpersonal and it was extrememly helpful in getting to know the docs and vice versa which helped when we called for med con, etc...
All around its a great idea but tough to implement and keep up on a regular basis as the 'rider' is often doing so for free. Another great thing that one of the services which i worked was we also did the reverse in the ER, kind of an exchange type deal and the medics also did ICU and OR as well.
Hope This Helps,
ACE844
-
:oops: i didnt check the date, just saw that it was in the "posts since last visit" category.
I know...just being facetious and mastabbas was the one who resus'd this thread.
ACE
-
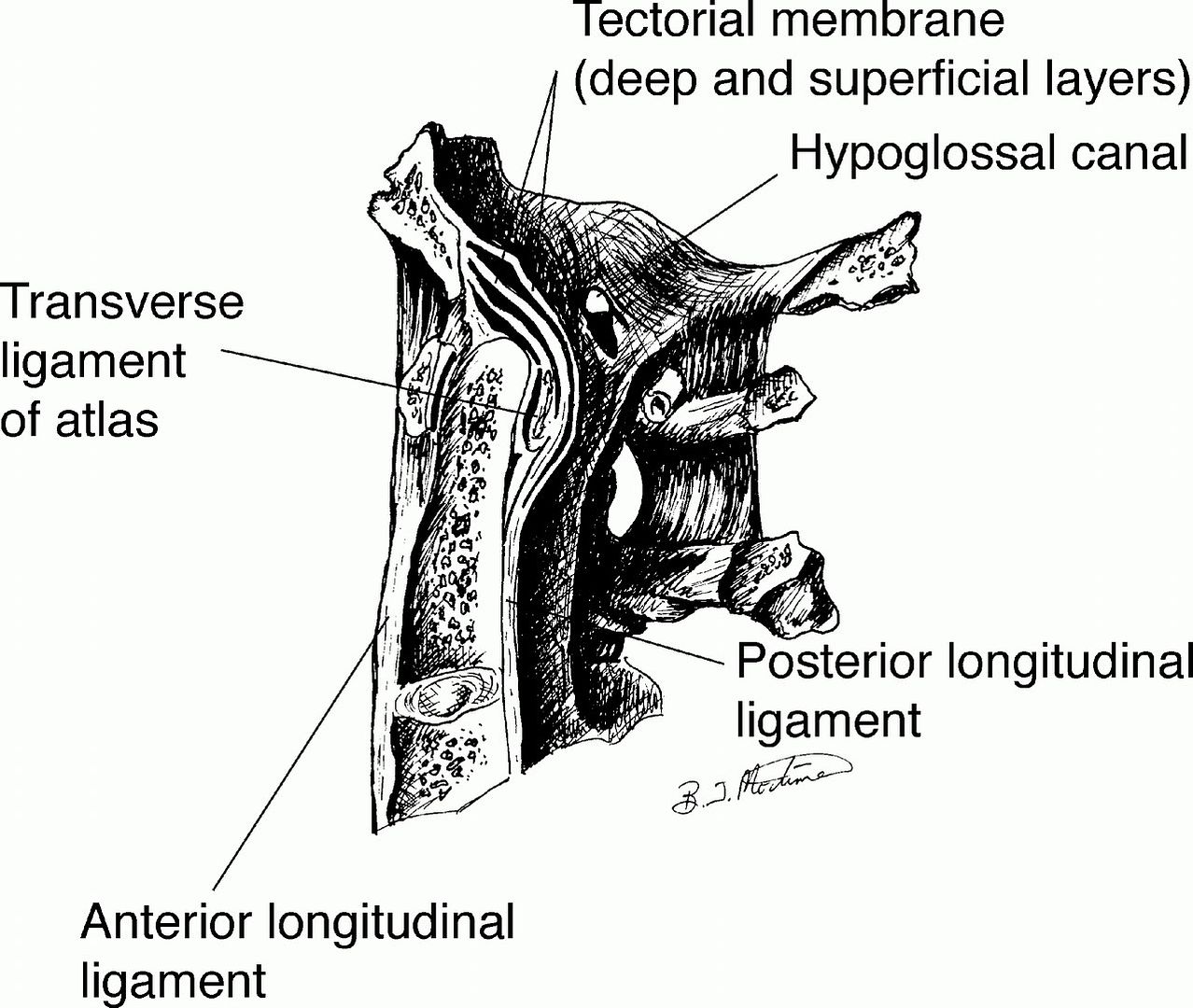
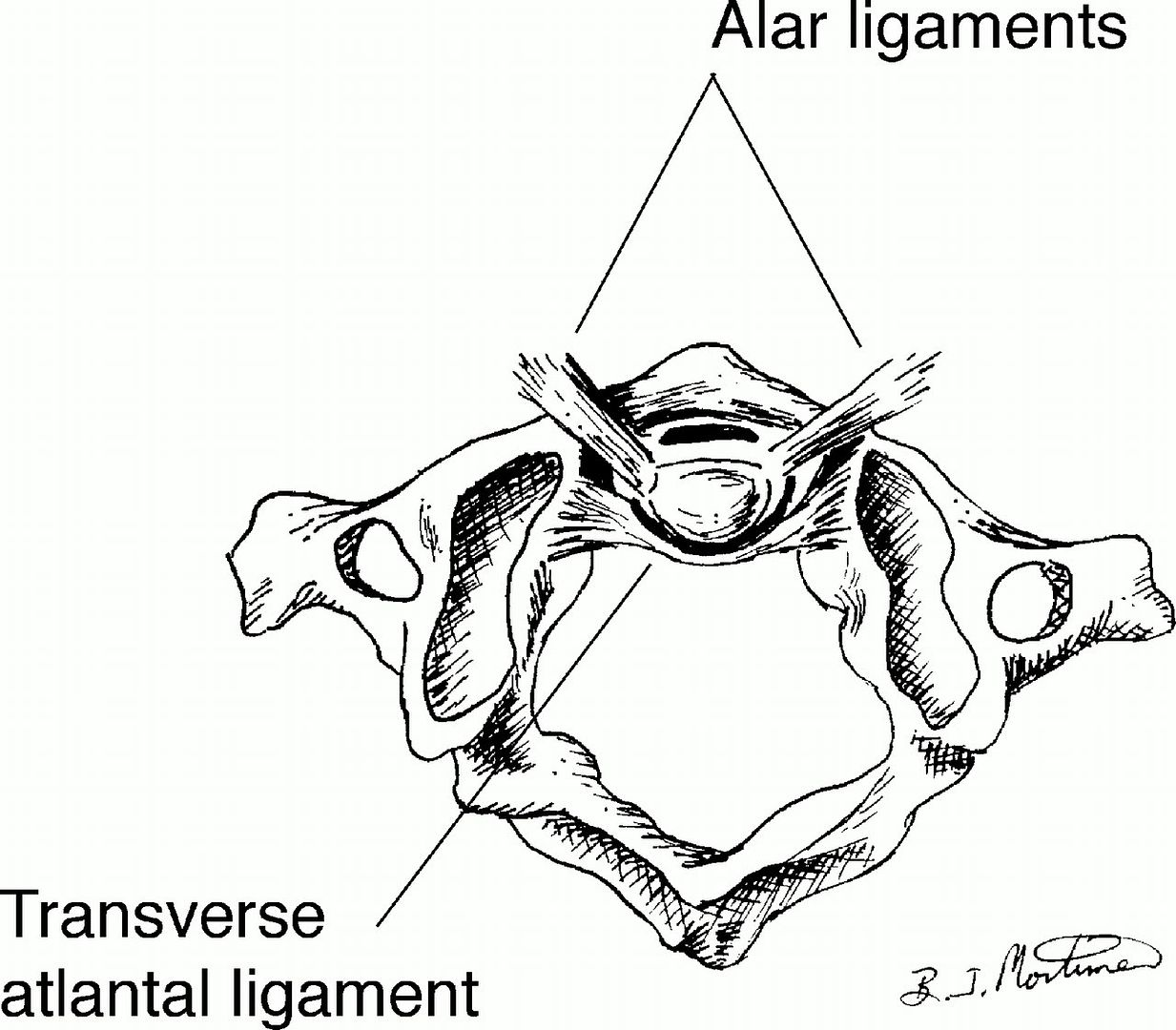
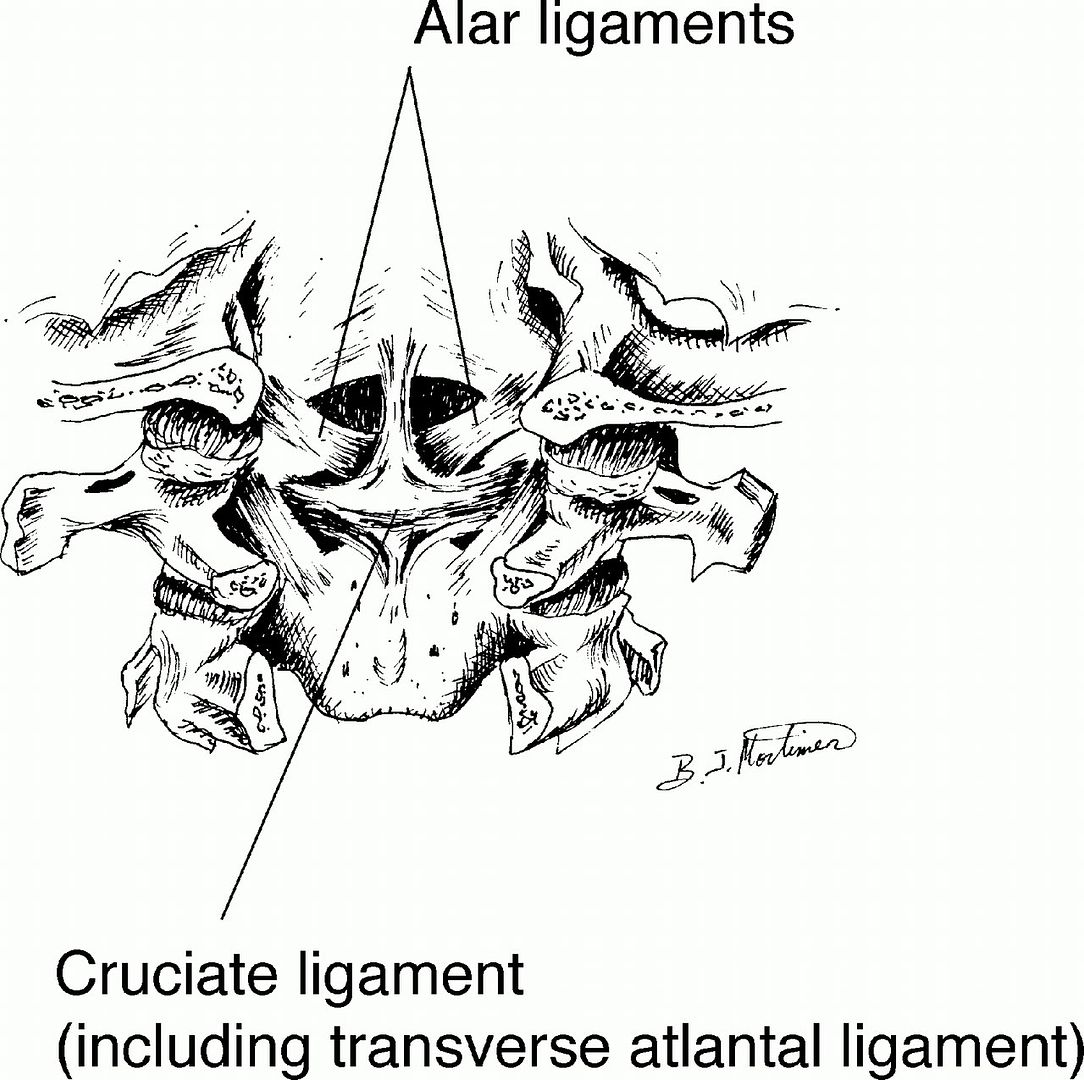
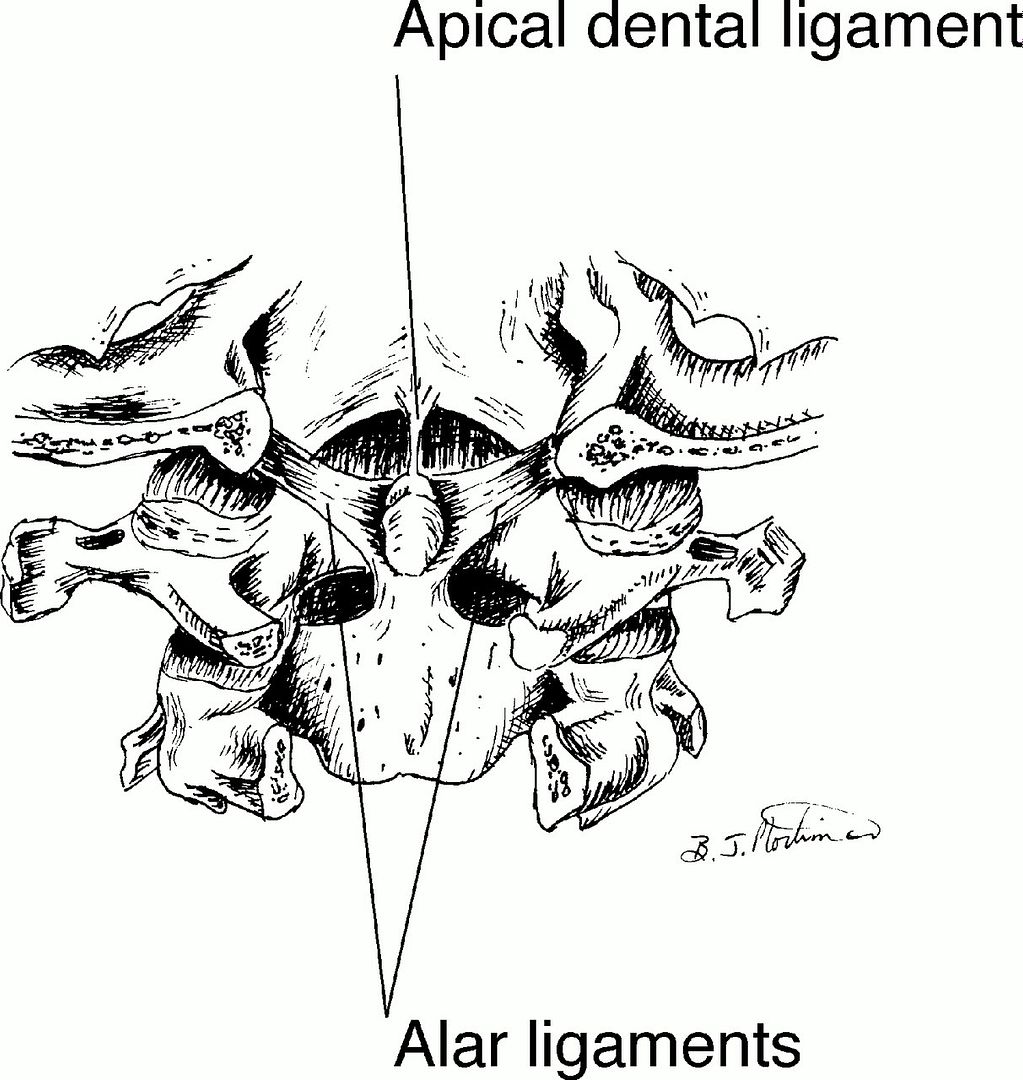
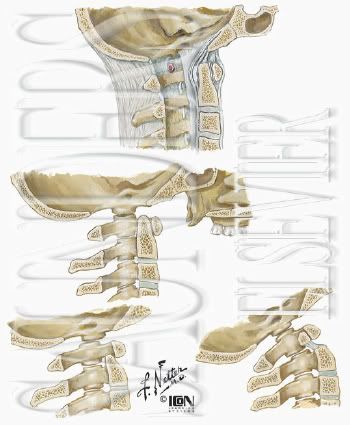
See this link: http://www.emedicine.com/orthoped/topic31.htm
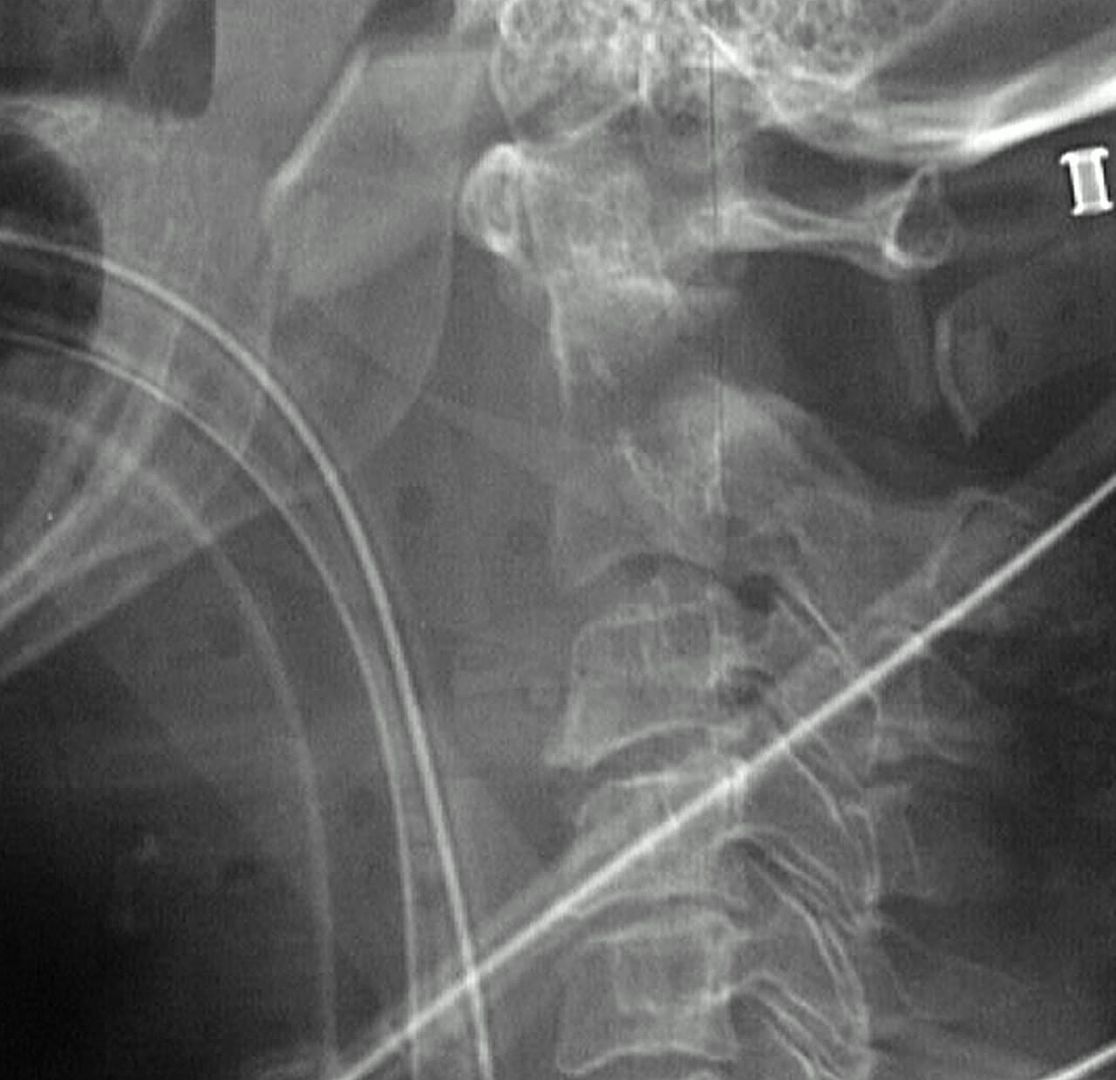
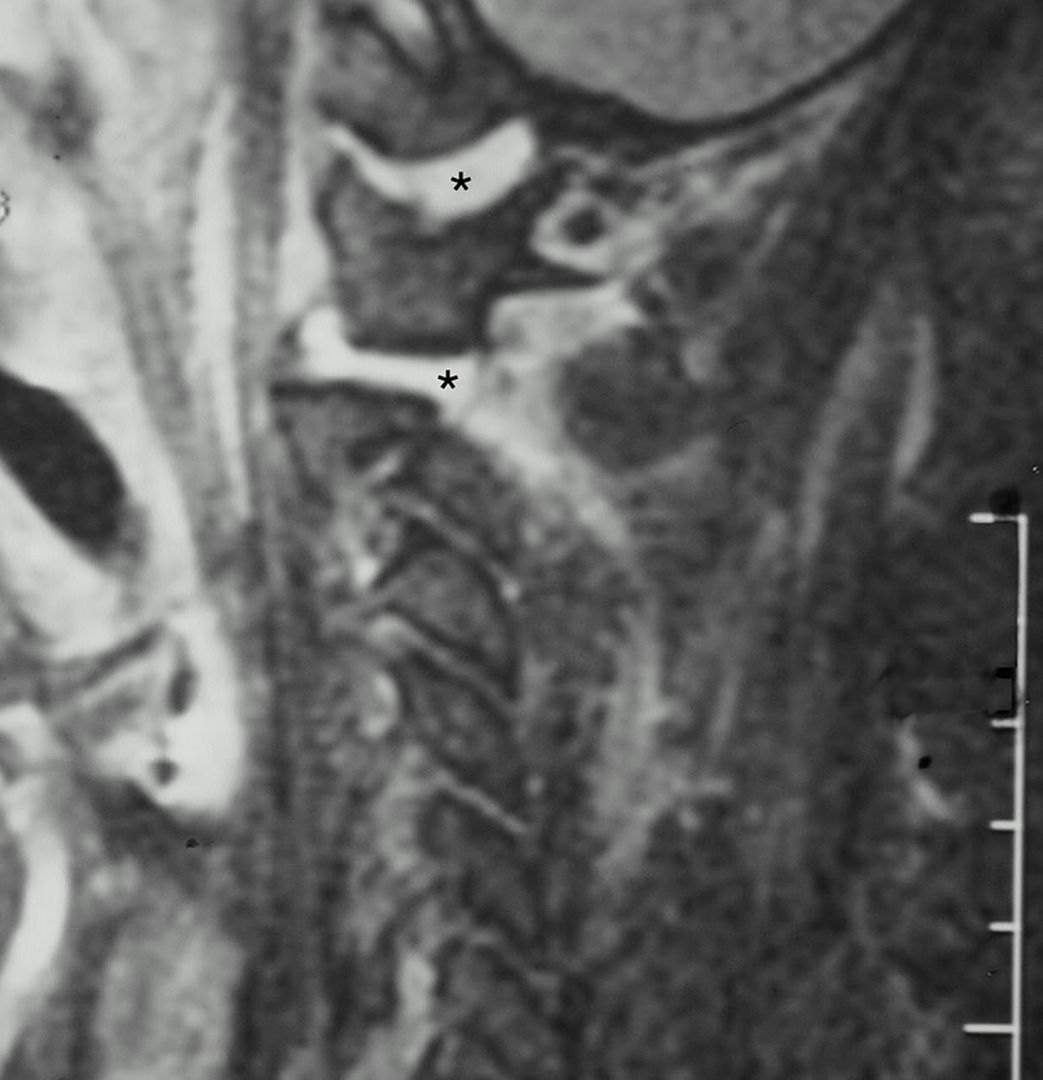
Below are pics of the anatomy and the last ones are of the pts injury...




-
to describe via an acronym you will probably recognize...FUBAR
-
-
 Welcome to EMTCITY!! [/font:779f918496]
Welcome to EMTCITY!! [/font:779f918496]
"jarjarjeffy,"

Please kindly read this
...http://www.emtcity.com/phpBB2/siterules.phpPlease take note of the area that mentions just how good a friend Google can be to you, and notice that in the upper Right hand corner of your screen is the 'SEARCH' button...
Please try to do some basic research before posting. Most fundamental questions have already been discussed multiple times on this site. Take a moment to use the "Search" function on this site to find previous discussions regarding your topic before starting a new topic.
Also, remember, www.Google.com is your friend! Many simple questions can be answered much more quickly on Google than by waiting for people to find, read, and then reply to your topic.
Read the entire topic before you reply. Chances are, somebody has already said the same thing you are about to say. If so, your input is probably no longer needed.
Do not hijack topics. Discussions should remain focused on the original poster's intended topic. If a separate topic or concern arises during the course of discussion, post that topic or concern in a new topic rather than sidetracking the original discussion.
Don't revive old, outdated topics unless you have something significant to add. If a topic has not been replied to in two or three months, it is probably because there is nothing left to add.
Choose a subject that describes your topic. When starting a new topic, it is important that you choose a subject title that accurately reflects the content of the thread. Do not make people guess what is in your topic. Threads posted with teaser titles like, "Guess what!," "I need help!," "What do you think?," "What would you do?," "What should be done?" or simply "Question!" will be deleted with extreme prejudice.
Give reasonable attention to your grammar. Although we want to maintain a casual atmosphere here, this is ultimately a PROFESSIONAL forum where members of the public are free to read and draw conclusions about us as a profession. There is an automatic spell checker provided on this forum. Please use it. Do not post messages that appear as if they were taken from a 13 year old girl's AOL chat. "You" is spelled YOU, not "u." "Whatever" is spelled WHATEVER, not "w/e." And punctuation is extremely important to those trying to understand your statements. If you are too pressed for time to type legibly and using punctuation and capitalization, then please come back later when you have more time. AND NEVER POST IN ALL CAPITAL LETTERS!
Edit the quotes in your replies. Don't re-quote the entire message of the post you are replying to. Either edit it down to only the relevant statement you are responding to, or delete the quotes altogether. If you don't know how to edit quotes, ask someone for help.
Do not post the same topic on several forums. Pick the most appropriate forum for your topic and post it there. Do not open the same discussion in multiple forums or threads. If you believe that your topic is so universally important that it needs to be in more than one forum, contact a moderator for assistance.
Do not "bump" your topic. Replying to your own topic to get it to the top is annoying. Try to have some patience; this is a bulletin board, not IRC. It may take some time (e.g., one or two days) before someone can answer your query or question.
Best of Luck,



ACE844

-
Imagine,
The analogy isn't all that much of a long shot. Because just the risks can be just as life threatening, or changin as maybe the case in either instance..
-
that's all we're askin. You popped the question for us to list stuff we've done be they big or small.
just remember, a journey of a million miles begins with just a simple step.
"Ruff,"
Sun tsu, tao tze, and all the others are on the psychic hotline...They told me to tell you..GREAT TIP!! :wink:
8) -
I'm going to suggest skipping the paramedic thing altogether.
Go to MEDICAL school instead, jock-o. Just remember where you came from.
Thanks for the vote of confidence, I haven't really thought about medschool all that much, certainly soemthing i will consider for the future though, thanks,
ACE
-
ACE I agree get your ass back in school and get your medic. But I think you have more important things to do in life and you have yet to start.
I'm working on finishing except I keep hitting speed bumps which has been extending my time to finish...work in progress, maybe I wouldn't have the 'non-personal situation' related delays if I had gone to a 'cook book' school, but even with all the extra time and headache, I wouldn't trade my education, or experiences in my program thus far for the world.. Thanks for the vote of confidence.
ACE
-
8) :shock: I have the best piece of anti-whacker equipment available....a pair of NIKEs!!
Currently we're running a world wide promotion!
-
High immune response seen with novel H5N1 avian influenza vaccine Story List
July 27, 2006
LONDON (Agence de Presse Medicale for Reuters Health) - A new H5N1 avian influenza vaccine may be filed with regulatory agencies in the coming months after study results showed the vaccine elicited a high immune response even at the lowest dose of antigen tested, vaccine-maker GlaxoSmithKline said Wednesday.
Early analysis of a clinical trial with 400 healthy volunteers showed that the vaccine elicited a strong seroprotective immune response in more than 80% of subjects who received 3.8 micrograms of antigen. "This level of seroprotection meets or exceeds target criteria set by regulatory agencies for registration of influenza vaccines," the company added in a statement.
"Efficacy results at these levels of antigen dosage have also not been reported for any other H5N1 vaccine in development to date, including those using other adjuvants such as alum," Glaxo continued.
J. P Garnier, GlaxoSmithKline's Chief Executive Officer, said: "These excellent clinical trial results represent a significant breakthrough in the development of our pandemic flu vaccine. This is the first time such a low dose of H5N1 antigen has been able to stimulate this level of strong immune response.
"There is still a lot more work to be done with this programme, but this validation of our approach provides us with the confidence to continue developing the vaccine, including assessment of its ability to offer cross-protection to variants of the H5N1 strain.
"All being well, we expect to make regulatory filings for the vaccine in the coming months," Garnier said.
The study was conducted in Belgium and involved adults between 18 and 60 years old who were vaccinated twice during the course of the trial. Four different levels of antigen dose were tested; 3.8 micrograms was the lowest dose assessed.
-
-
(The Lancet Infectious Diseases
Volume 6 • Number 2 • February 2006
Copyright © 2006 Elsevier
Newsdesk
Oseltamivir resistance raises bird flu concerns
Helen Pilcher
--------------------------------------------------------------------------------
PII S1473-3099(06)70368-1)
Two Vietnamese patients infected with the H5N1 avian influenza strain developed resistance to the antiviral drug oseltamivir (Tamiflu) before their deaths. The finding raises concerns over the drug's use, and reinforces the need for better therapies to avert a global bird flu pandemic.Menno de Jong (Oxford University Clinical Research Unit, Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam) and colleagues analysed throat swabs taken from eight Vietnamese patients infected with the H5N1 strain of avian influenza. Viral isolates taken during and after the standard oseltamivir treatment regimen (two 75 mg doses per day for 5 days) were tested for a genetic mutation known to render influenza viruses resistant to oseltamivir.
The mutation was found in two patients. Both died, even though one received treatment speedily, within 24 hours of symptoms developing. Two other patients who did not carry the mutation also died. “With four patients surviving, the good news is that oseltamivir works in a proportion of patients”, says de Jong. “The bad news is that resistance to the drug may not be that rare.”
In one patient the development of resistance coincided with a dramatic worsening of symptoms, suggesting that resistance contributes directly to disease progression. “We need to minimise the development of resistance”, says de Jong.
One approach could be to increase the dosage. Higher doses may be better at stunting viral replication, so limiting the likelihood of oseltamivir-resistant mutations occurring. Another option may be to offer oseltamivir alongside other antiviral drugs. Zanamivir (Relenza), for example, is thought to be effective against oseltamivir-resistant influenza virus. However, the downside of zanamivir is that it is only available in inhaled form, and so does not offer the systemic protection thought necessary against avian flu.
But oseltamivir is still the main anti-influenza drug recommended by WHO, and many believe that there should be a supply in every medicine cabinet. This scenario is potentially dangerous, says Anne Moscona (Weill Medical College, Cornell University, New York, USA). Misuse of the oseltamivir could rob us of the drug's advantages by favouring the emergence of oseltamivir-resistant influenza virus.
With the continued global spread of avian flu among poultry and wild birds, concerns remain that the virus may trigger a human pandemic. But before this happens, the virus will have to change further—either by mutating or recombining with another virus—and become able to spread directly between people. But “it is impossible to say if this new virus would also become resistant to Tamiflu”, says de Jong. “We'll just have to wait and see.”
(Bird flu kills Thai youth amid new outbreaks Story ListJuly 27 @ 2006
By Darren Schuettler
BANGKOK (Reuters))
A 17-year-old Thai has died of the H5N1 bird flu virus, the country's first death this year as it battles fresh outbreaks of the disease, a senior health official said on Wednesday.The young man died on Monday in the northern province of Pichit, where authorities have slaughtered hundreds of birds and restricted poultry movement in a bid to stamp out Thailand's first outbreak in eight months.
"The final lab test confirmed that he died of bird flu," Kamnuan Ungchusak, head of the Health Ministry's epidemiology bureau, told Reuters by telephone from the hospital where the youth died.
He is believed to have caught the virus while helping his father bury dead chickens last week.
The father showed no flu-like symptoms of the virus which has killed 15 Thais since it swept across parts of Asia in 2003. The last Thai victim, a five-year-old boy, died in December last year.
"We have quarantined the family and there is no report of a new case yet," Kamnuan said.
Not including this latest death, bird flu has killed 133 people worldwide since the virus re-emerged in Asia in 2003, the World Health Organization says.
At present, H5N1 remains essentially a disease of birds and is hard for people to catch.
But scientists fear the virus could mutate into a form that spreads easily among humans and trigger a pandemic in which millions could die.
The outbreak in Pichit, one of seven high-risk Thai provinces where surveillance was stepped up this month, was confirmed by the Agriculture Ministry on Tuesday, but the source of the infection was not known.
The U.N. Food and Agriculture Organization (FAO) called for an "intense investigation" of the outbreak. It said Thailand had done a good job in fighting the virus so far, but it may need to fine-tune its surveillance.
"Clearly they have pushed this thing down to the level of almost non-existence, but either it's been reintroduced or it has persisted and at such a low level it did not cause any significant blips," Laurence Gleeson, a senior FAO official in Bangkok, told Reuters.
Thailand was slow to respond to bird flu when it first began ravaging poultry flocks in late 2003, badly damaging what was the world's fourth largest chicken export industry.
Critics accused the government of trying to cover up this latest outbreak, a charge denied by Livestock Department officials who said they had informed the public as soon as tests confirmed the presence of H5N1.
Gleeson said the FAO, which has stressed the need for rapid and transparent reporting of outbreaks, had no complaints about Thailand's reporting procedures. (Additional reporting by Nopporn Wong-Anan)
(The Lancet Infectious DiseasesVolume 6 • Number 5 • May 2006
Copyright © 2006 Elsevier
Newsdesk
Human-to-human spread of H5N1—location may matter
Jane Bradbury
--------------------------------------------------------------------------------
PII S1473-3099(06)70450-9)
The H5N1 avian influenza virus attaches predominantly to cells deep within the human respiratory tract, report two research teams. Although both senior researchers— Thijs Kuiken (Erasmus Medical Center, Rotterdam, Netherlands) and Yoshihiro Kawaoka (University of Wisconsin-Madison, Madison, WI, USA)—stress that many factors affect human-to-human transmission of H5N1, the absence of attachment in the upper respiratory tract might, they suggest, contribute to the current inefficiency of this process.More than 100 people have been infected by H5N1 but this highly pathogenic virus has rarely, if ever, passed between people. Indeed, given its widespread occurrence within bird flocks, relatively few people have caught H5N1 from birds. Could it be, therefore, that only people who get bird flu have receptors on their cells for H5N1? Flu viruses attach to sialosaccharides on their host cells through haemagglutinin. In human flu viruses, this protein spike recognises sialic acid linked to galactose by an ɑ2,6 linkage; avian flu haemagglutinin recognises ɑ2,3-linked sialosaccharides.
To investigate whether human cells lack H5N1 receptors, Kawaoka's team stained material from the human respi ratory tract with lectins specific for these two linkages. They found that cells in the upper respiratory tract contain receptors for human flu viruses but only cells deep in the lungs express avian virus receptors. This receptor distribution, which the researchers confirmed by examining the binding of avian and human flu viruses, provides a partial explanation for H5N1's poor human-to-human transmission, says Kawaoka. “Because H5N1 viruses don't grow in the upper portion of the respiratory tract, they cannot be readily transmitted by coughing and sneezing.”
Kuiken and his team also investigated H5N1 virus attachment to the human respiratory tract. “We wanted to understand why H5N1 causes pneumonia”, explains Kuiken, “and like Kawaoka, we found that this virus attaches to alveolar type II pneumocytes and to non-ciliated cuboidal epithelial cells in the terminal bronchioles”. The attachment to type II pneumocytes, says Kuiken, provides new insights into the pathogenesis of H5N1 because these cells normally repair damaged lung tissue. But, he cautions, “our results only suggest, rather than prove, an explanation for the poor spread of H5N1 between people”.
“These two papers help to define the receptor distribution within the human respiratory tract for avian viruses like H5N1”, comments flu expert Frederick Hayden (University of Virginia, Charlottesville, VA, USA), “and they fit well with the clinical observation that H5N1 can cause severe primary viral pneumonia. But the idea that this receptor distribution explains poor person-to-person transmission is only speculation.” And, although mutations in the H5N1 haemagglutinin that change its binding pattern to human cells might take H5N1 a step closer to causing a human pandemic, other adaptations will also be required, conclude Hayden, Kuiken, and Kawaoka.

Here's an interesting position paper on Rural EMS
in General EMS Discussion
Posted
Here's an interesting position paper on Rural EMS::
This paper bring to light many ideas and solutions which we have been discussing for some time here. What do you all think, is this a decent foundation for future change?
ace844
http://www.nemsma.org/Portals/3/EMSworkforce.pdf